
Spoiler alert: A tiny electrical device clipped to your ear might one day help calm the raging storm of inflammation that follows a serious brain injury. The researchers behind the MINT trial haven't proven it yet - that's literally the whole point of the trial - but the science that got them here is genuinely fascinating, and the implications for communities that bear the heaviest burden of traumatic brain injury are worth paying attention to.
Now let me back up and explain how we got to the point where "electrocute the ear, save the brain" became a legitimate sentence in a medical journal.
Traumatic Brain Injury: The Quiet Epidemic
Traumatic brain injury (TBI) affects roughly 69 million people worldwide every year. Let that number sit with you for a second. That's nearly the entire population of the United Kingdom getting their bell rung annually. In the U.S. alone, TBI contributes to about 190 deaths per day, and those statistics land hardest on communities already dealing with stacked disadvantages - low-income neighborhoods, communities of color, rural areas with limited access to trauma centers, and unhoused populations (Simon et al., 2017).
Here's the thing about TBI that makes it particularly nasty: the initial injury is just the opening act. After the skull absorbs the hit, the brain launches an inflammatory response that's supposed to be helpful - think of it as your immune system's version of calling 911. But in moderate to severe TBI (measured by a Glasgow Coma Scale score of 3-12, where lower is worse), that inflammatory response goes completely off the rails. It's like calling the fire department and they show up with flamethrowers. This secondary inflammation can continue damaging brain tissue for days and weeks after the original injury, turning a bad situation into a catastrophic one.
And despite decades of research, we still don't have a great pharmaceutical option for reining in that runaway neuroinflammation. Pretty much every promising drug has face-planted in clinical trials. Which brings us to... the ear thing.
The Vagus Nerve: Your Body's Built-In Chill Button
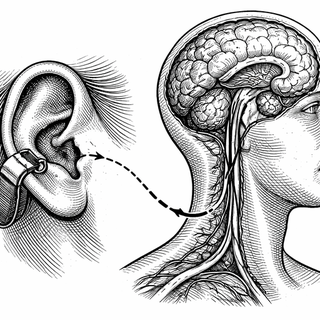
The vagus nerve is the longest cranial nerve in your body, wandering from your brainstem all the way down to your gut like a biological superhighway. Among its many jobs, it runs what scientists call the "cholinergic anti-inflammatory pathway" - essentially a hardwired system for telling your immune system to calm down. Stimulating the vagus nerve has been shown to reduce pro-inflammatory cytokines like TNF-alpha and IL-6, which are exactly the troublemakers that go haywire after a brain injury (Yap et al., 2020).
Traditionally, vagus nerve stimulation (VNS) required surgically implanting a device around the nerve in your neck. Effective? Sure. Practical for someone who just arrived in the ER with a severe brain injury? Not so much. You generally want fewer surgeries for your acute trauma patient, not more.
Enter transcutaneous auricular vagus nerve stimulation - taVNS for those of us who value our breath. It turns out a branch of the vagus nerve surfaces at a specific spot in your ear called the cymba conchae (the little ridge in the bowl of your outer ear). By placing a small electrode there and delivering gentle electrical pulses through the skin, you can activate the vagus nerve without a single incision. It's basically a TENS unit for your ear, and early research suggests it can tap into that same anti-inflammatory superhighway (Badran et al., 2018).
The MINT Trial: First, Do No Harm (Then Maybe Do Some Good)
The MINT trial - Modulating Inflammation in Neuro-Trauma - is a single-site, prospective, randomized, double-blind, sham-controlled pilot study. If that string of adjectives made your eyes glaze over, here's the translation: this is a carefully designed early-stage study where neither the patients nor the clinicians know who's getting the real treatment versus a fake version, which is the gold standard for minimizing bias.
Participants are patients with moderate to severe TBI (GCS 3-12) who get randomized to receive either active taVNS or sham stimulation using an identical-looking device. The primary question isn't even "does this work?" - it's "is this safe and feasible to do in an acute TBI setting?" That might sound anticlimactic, but in clinical research, it's the responsible first step. You don't skip to the finish line when you're dealing with people who have serious brain injuries.
The secondary objectives are where it gets interesting: the team will measure serum inflammatory and neuronal injury biomarkers - the molecular breadcrumbs that tell you whether inflammation is actually being dialed down - and track functional outcomes using the Extended Glasgow Outcome Scale at hospital discharge.
Why This Matters for Health Equity
Here's where my public health heart starts beating faster. If taVNS proves safe and eventually effective for acute TBI, the equity implications are enormous. Consider the current landscape: the best TBI outcomes require rapid transport to a Level I trauma center, access to neurosurgery, extended ICU stays, and months of rehabilitation. That's a resource-intensive pipeline that systematically disadvantages rural communities, uninsured patients, and under-resourced hospitals.
taVNS is non-invasive, portable, relatively inexpensive, and doesn't require a neurosurgeon to administer. A community hospital ER doc could potentially apply it. A military medic in the field could carry one. The device doesn't need a pharmacy supply chain or cold storage. If the science holds up, this is exactly the kind of intervention that could narrow the gap between who gets optimal TBI care and who doesn't.
Animal studies have already shown that vagus nerve stimulation after TBI can reduce brain edema, lower inflammatory marker levels, and improve neurological outcomes (Huffman et al., 2019). The jump from rodent ears to human ears is never guaranteed - mice have been cured of basically everything at this point - but the mechanistic foundation here is solid enough to justify a careful human trial.
The Road Ahead
Let's be real: this is a pilot study. It's designed to answer whether we can do this safely, not whether it definitively works. Even in the best-case scenario, we're looking at years of larger trials before taVNS becomes a standard TBI treatment. The history of TBI therapeutics is littered with promising interventions that didn't survive Phase III trials, and healthy skepticism is warranted.
But there's something genuinely exciting about an approach that leverages the body's own anti-inflammatory wiring, requires no surgery, and could theoretically be deployed anywhere from a university hospital to a rural clinic. The MINT trial isn't going to change TBI care overnight. What it might do is crack open a door that a lot of very motivated researchers can push through - and that's how progress actually happens.
In the meantime, I'll be over here, unreasonably excited about ear stimulation. Which is a sentence I never expected to write in a professional context.
Disclaimer: This blog post is for informational and educational purposes only and does not constitute medical advice. Clinical trial information is based on publicly available data and may be updated as the study progresses. Always consult healthcare professionals for medical decisions.
References:
-
Simon, D. W., et al. (2017). The far-reaching scope of neuroinflammation after traumatic brain injury. Nature Reviews Neurology, 13(3), 171-191. https://doi.org/10.1038/nrneurol.2017.13
-
Yap, J. Y. Y., et al. (2020). Critical Review of Transcutaneous Vagus Nerve Stimulation: Challenges for Translation to Clinical Practice. Frontiers in Neuroscience, 14, 284. https://doi.org/10.3389/fnins.2020.00284
-
Badran, B. W., et al. (2018). Neurophysiologic effects of transcutaneous auricular vagus nerve stimulation (taVNS) via electrical stimulation of the tragus. Brain Stimulation, 11(3), 492-500. https://doi.org/10.1016/j.brs.2017.12.009
-
Huffman, W. J., et al. (2019). Modulation of neuroinflammation and memory dysfunction using percutaneous vagus nerve stimulation in mice. Brain Stimulation, 12(1), 19-27. https://doi.org/10.1016/j.brs.2018.10.005
-
ClinicalTrials.gov. MINT: Modulating Inflammation in Neuro-Trauma. Identifier: NCT07510074. https://clinicaltrials.gov/study/NCT07510074