
Deep beneath your scalp, osteoblasts are performing the most thankless construction job in biology. These bone-building cells crawl along the inner table of your skull, depositing hydroxyapatite crystals with the quiet diligence of municipal road workers filling potholes at 3 AM. They lay down collagen scaffolds, mineralize them, and maintain the curved, layered architecture of cranial bone - a composite so elegantly engineered that it's simultaneously rigid enough to protect your brain and compliant enough to absorb a glancing blow. Now imagine a chunk of that architecture goes missing. Trauma, tumor resection, decompressive surgery. The osteoblasts show up to work and find the job site just... gone. What do you give them to build on?
That question is the entire field of cranioplasty in a nutshell. And for decades, the answer has been unsatisfying.
The "Good Enough" Problem
Cranioplasty - the surgical repair of skull defects - has been practiced since at least the 16th century, which should tell you something about how long we've been trying to get it right. The modern options boil down to two imperfect choices: titanium mesh or PMMA (polymethyl methacrylate, essentially medical-grade acrylic).
Titanium is biocompatible and strong, but it's roughly five times stiffer than cranial bone. This stiffness mismatch creates what engineers call "stress shielding" - the implant hogs all the mechanical load, and the surrounding bone, suddenly unemployed, starts to resorb. It's the skeletal equivalent of a government program that's so efficient it puts the people it was meant to help out of work.
PMMA, meanwhile, is cheaper and easier to mold, but it's essentially inert plastic. Bone cells look at it the way a cat looks at a cucumber - with deep suspicion and zero interest in integration. PMMA implants can loosen over time, and they lack the biological handshake that tells surrounding tissue "yes, I belong here."
Neither material was designed to mimic the sandwich structure of actual cranial bone, which features dense cortical layers on the outside and spongy diploe in the middle. We've been asking patients to accept skull patches that feel nothing like skull.
Enter the Sandwich
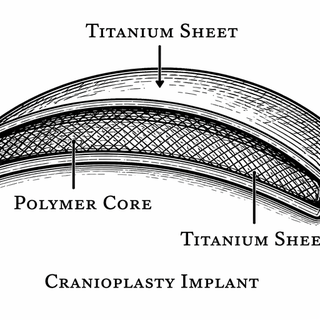
A new study published in 2025 presents a genuinely clever rethinking of the problem. Researchers designed a bioactive sandwich composite - Ti/polymer/Ti - that stacks two thin titanium sheets around a tunable polymer core, mimicking the layered architecture of natural cranial bone (Pubmed).
The "second-generation" part is telling. The team's earlier work used a straight PMMA core, which, as we discussed, has all the biological charm of a plastic cafeteria tray. This time, they replaced it with P(MMA-co-...) copolymers - essentially PMMA remixed with additional monomers that let engineers dial in the mechanical properties like adjusting an equalizer. Want more flexibility? Tweak the copolymer ratio. Need the implant stiffer in one region? Adjust accordingly.
The result is a composite whose stiffness can be tuned to match cranial bone rather than dramatically overshoot it. The titanium outer layers provide the strength and biocompatible surface that bone cells already know how to attach to, while the polymer core handles energy absorption and compliance. It's a materials science answer to a question biology has been asking for a very long time.
Why "Scalable" Is the Quiet Revolution
Here's where the health policy nerd in me gets excited. Medical materials research is littered with gorgeous lab-bench prototypes that never survive contact with manufacturing economics. You can design the perfect implant, but if producing each one requires a PhD student, a clean room, and a small prayer circle, it's not going to help the roughly 30,000 patients who undergo cranioplasty in the U.S. each year.
The researchers explicitly addressed scalable fabrication, meaning these composites can be manufactured using existing industrial processes rather than boutique lab techniques. The Ti/polymer/Ti architecture lends itself to roll-bonding and thermoforming - processes that factories already know how to do. This isn't a material that needs its own startup. It needs a production line.
For anyone who has watched a promising biomaterial languish in the "valley of death" between bench and bedside - and that valley has its own zip code at this point - the emphasis on manufacturability is quietly radical.
Bioactivity: Making Friends With Bone
The "bioactive" descriptor in the title isn't marketing fluff. The titanium surfaces can be treated to promote osseointegration - the process by which living bone forms a direct structural and functional connection with the implant surface. Those osteoblasts from our opening scene? Give them a properly textured titanium surface and they'll colonize it like it's free real estate.
This matters enormously for long-term outcomes. An implant that integrates with surrounding bone becomes part of the patient's anatomy. One that just sits there, mechanically clamped in place, is a perpetual infection risk and a candidate for eventual failure. The difference between "tolerated by the body" and "welcomed by the body" is the difference between a tenant and a homeowner.
What This Means for the Regulatory Crowd
Composite implants occupy an interesting regulatory niche. They're not purely metallic (well-understood pathway) and not purely polymeric (another well-understood pathway). They're both, which means regulatory bodies like the FDA will need to evaluate mechanical performance, biocompatibility, degradation behavior, and manufacturing consistency for a material that behaves differently depending on which layer you're asking about.
This is the kind of thing that makes regulatory scientists reach for stronger coffee. But it's also exactly the kind of challenge that, once navigated, opens the door for an entire class of tunable sandwich implants - not just for cranioplasty, but potentially for any skeletal repair where mechanical matching matters.
The Bigger Picture
We're in a moment where materials science is finally catching up to the complexity of the problems surgeons face daily. For too long, the choice has been "pick the least bad option from Column A." Research like this suggests a future where implants are engineered from the ground up to behave like the tissue they're replacing - mechanically, biologically, and architecturally.
It won't happen overnight. Clinical trials, regulatory review, manufacturing scale-up, and reimbursement coding all stand between a lab result and a patient outcome. That pipeline is long, expensive, and occasionally absurd. But the engineering foundation being laid here is solid, and the emphasis on practical manufacturability suggests a team that understands the distance between "it works" and "it's available."
Your osteoblasts deserve better building materials. This might be a step toward giving them some.
This blog post discusses research findings and should not be taken as medical advice. If you have concerns about cranioplasty or cranial reconstruction, please consult a healthcare provider. Research discussed here represents ongoing scientific investigation and clinical validation is still in progress.
All images used in this post are decorative illustrations only and do not represent or reflect the accuracy, reality, or correctness of the referenced research.
Primary Source: Design and Scalable Fabrication of Bioactive Ti/Polymer/Ti Sandwich Composites with Controlled Mechanics for Cranioplasty. PubMed. 2025. PMID: 41941542