
**By You spend decades using it without a second thought - walking, running, pretending you're still athletic at your company softball game - and then one day it just... pops. Like an overstretched rubber band on a lobster claw. Except the lobster claw is your leg, and now you're looking at surgery, months of rehab, and the very real possibility that your calf muscle will never quite cook back to its original consistency.
Enter Project Tendura, a new clinical trial (NCT07498166) that wants to know whether partially cutting off blood flow to your leg while you exercise might actually be the secret ingredient for getting your muscle back after Achilles tendon repair. Yes, you read that right. Tourniquets. On purpose. During rehab.
Welcome to blood flow restriction training, or BFR-RT, the rehabilitation equivalent of pressure-cooking your recovery.
What Exactly Snaps When Your Achilles Goes
The Achilles tendon is the thickest, strongest tendon in the human body, connecting your calf muscles - the gastrocnemius and soleus - to your heel bone. It handles forces of up to 12 times your body weight during running. It is, by any engineering standard, a magnificently over-spec'd piece of biological hardware.
And yet roughly 18 per 100,000 people rupture it every year, with incidence climbing steadily among recreational athletes aged 30-50. The typical story involves a weekend warrior making a sudden push-off movement, hearing a sound like a gunshot, and then discovering that their foot has become a floppy, unresponsive appendage. Surgical repair stitches the tendon back together, but here's the problem: the calf muscle behind it atrophies fast. Really fast. We're talking 10-20% loss of muscle cross-sectional area within weeks. And standard rehab, while effective, often leaves patients with persistent strength deficits at one year or beyond.
It's like reassembling a gourmet burger but forgetting to season the patty. The structure is there, but the substance is lacking.
The Pressure Cooker Principle: How BFR Works
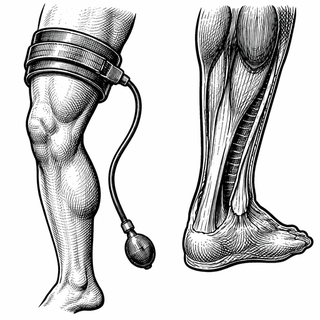
Blood flow restriction training is one of those ideas that sounds mildly unhinged until you look at the physiology. The concept: you wrap a specialized pneumatic tourniquet around the upper portion of a limb, inflate it to a calibrated pressure - typically 40-80% of the limb's total occlusion pressure - and then perform exercises at laughably low loads. We're talking 20-30% of your one-rep max. Weights that would normally do about as much for hypertrophy as stirring a pot of soup.
But here's where it gets interesting. By restricting venous blood outflow while allowing arterial inflow, BFR creates a localized metabolic environment that mimics high-intensity training. Lactate accumulates, growth hormone spikes, and your muscle fibers get recruited as if you were grinding through a heavy set - all without the mechanical stress that could compromise a freshly repaired tendon. A 2019 consensus statement from Patterson et al. laid out the physiological framework pretty thoroughly, noting that BFR essentially lets you get a steak-level anabolic stimulus from a side-salad-level load (DOI: 10.3389/fphys.2019.00533).
Hughes et al. published a systematic review in the British Journal of Sports Medicine showing that BFR training in clinical musculoskeletal rehab settings produced meaningful improvements in muscle strength and hypertrophy compared to low-load training alone (DOI: 10.1136/bjsports-2016-097071). And Ladlow et al. demonstrated in a single-blind RCT that low-load BFR improved clinical outcomes in military personnel undergoing musculoskeletal rehab (DOI: 10.3389/fphys.2018.01269).
The evidence base is growing. What's been missing is a rigorous, three-arm trial specifically targeting Achilles tendon rupture patients. Which is exactly what Project Tendura is serving up.
Inside the Trial: Three Groups, One Ruptured Tendon
The study design is refreshingly clean. Adults who've undergone primary surgical repair of an acute Achilles tendon rupture get randomized into one of three groups:
- BFR-RT plus standard physical therapy - the real deal, with a personalized tourniquet system calibrated to each patient's limb occlusion pressure
- Sham BFR-RT plus standard physical therapy - same tourniquet, same setup, but inflated to a pressure too low to actually restrict blood flow (the rehab equivalent of decaf)
- Standard physical therapy alone - the control group, doing conventional rehab with no cuff at all
That sham group is the engineering detail I appreciate most. One of the persistent criticisms of BFR research has been inadequate blinding. It's hard to placebo-control a tourniquet squeezing your thigh. But calibrating a sham cuff to sub-therapeutic pressures is about as close as you can get, and it lets the researchers tease apart the psychological "I'm getting a special treatment" effect from the actual physiological response.
What They're Measuring (And Why It Matters)
The primary outcome is ankle plantarflexion strength - basically, how hard you can push your foot down - measured using the Fysiometer platform. This is the metric that correlates most directly with return-to-sport capability and is where Achilles rupture patients tend to have the most stubborn deficits.
Secondary outcomes include ultrasound imaging of the gastrocnemius-soleus complex (to directly measure muscle cross-sectional area) and patient-reported outcome measures for pain and function. Follow-ups run at 6 weeks, 3 months, 4.5 months, 6 months, and 12 months post-op. That 12-month endpoint is key, since it tells us whether any early gains from BFR actually stick or fade like last season's fitness resolution.
Why I'm Cautiously Optimistic (And Still Skeptical)
I've covered enough "revolutionary" rehab modalities to know that the gap between "promising mechanism" and "actually changes outcomes at scale" is roughly the width of the Grand Canyon. BFR has solid physiological plausibility, decent supporting literature, and growing adoption in sports medicine clinics. But the Achilles rupture population is specific. These patients are dealing with a surgically repaired structure that needs to be loaded progressively without being overcooked. The tourniquet pressure calibration, the exercise protocols, the timing relative to tissue healing - getting this recipe right requires precision.
What gives me confidence in Project Tendura is the methodological rigor: three-arm design, sham control, objective strength testing, imaging-based muscle assessment, and a full year of follow-up. This isn't a pilot study in 12 college athletes. This is a trial designed to actually answer the question.
If the results pan out, the clinical implications are significant. Achilles tendon rupture rehab could get a well-validated tool that accelerates muscle recovery without increasing mechanical risk to the repair. For the estimated 30,000+ Americans who rupture their Achilles annually, that's the difference between getting back to full function and permanently walking around with a calf that looks like it belongs to someone else's leg.
The Bottom Line
BFR training for post-surgical Achilles rehab is a genuinely clever application of exercise physiology. Project Tendura is asking the right questions with the right study design. Whether the data cooperates remains to be seen - biology has a habit of ignoring our hypotheses - but this is exactly the kind of trial that moves a field from "sounds reasonable" to "here's the evidence."
I'll be watching this one simmer. Sometimes the slow cooker produces the best results.
This article is for informational and educational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider regarding any medical condition or treatment. Clinical trial participation should be discussed with your physician.
Trial Reference: Project Tendura: The Impact of Blood Flow Restriction Resistance Training (BFR-RT) in Patients With Achilles Tendon Rupture (ATR) Repair. ClinicalTrials.gov Identifier: NCT07498166
Citations:
-
Patterson SD, Hughes L, Warmington S, et al. Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Front Physiol. 2019;10:533. DOI: 10.3389/fphys.2019.00533
-
Hughes L, Paton B, Rosenblatt B, Gissane C, Patterson SD. Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis. Br J Sports Med. 2017;51(13):1003-1011. DOI: 10.1136/bjsports-2016-097071
-
Ladlow P, Coppack RJ, Dharm-Datta S, et al. Low-Load Resistance Training With Blood Flow Restriction Improves Clinical Outcomes in Musculoskeletal Rehabilitation: A Single-Blind Randomized Controlled Trial. Front Physiol. 2018;9:1269. DOI: 10.3389/fphys.2018.01269