
Ever tried to hang a heavy shelf on drywall without finding a stud? You know that sinking feeling when the anchor just spins uselessly, and your beautiful IKEA purchase crashes to the floor along with your dignity? Well, dental implants face a remarkably similar problem. Without enough solid bone to anchor into, even the most sophisticated titanium implant is basically a very expensive loose screw. And that's exactly where maxillary sinus augmentation comes in - it's essentially adding studs to your jaw's drywall.
What's All This About Sinus Lifting?
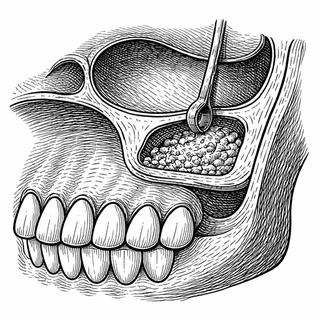
Here's a fun anatomical fact that might ruin your day: the maxillary sinuses - those air-filled cavities behind your cheekbones - sit right above your upper back teeth. When those teeth go missing (whether from extraction, decay, or an unfortunate encounter with a jawbreaker that lived up to its name), the bone beneath them starts to shrink. Meanwhile, the sinus above starts to expand downward, like a nosy neighbor slowly encroaching on your property line.
This leaves patients with a thin shelf of bone that's about as useful for implant placement as tissue paper is for building a house. The solution? A procedure called maxillary sinus augmentation, or more dramatically, a "sinus lift." Surgeons access the sinus through a lateral window technique (think of it as cutting a tiny doggy door in the side of your jaw), gently lift the sinus membrane, and pack the space with bone graft material. Six months later - voilà - you've got yourself some brand new bone real estate ready for implant construction.
The MSA-BGC Study: A Tale of Two Jaws
A new clinical trial (NCT07512011) is taking this renovation project to the next level by asking a question that's been nagging researchers for years: does the specific recipe of bone graft material actually matter?
The MSA-BGC Study (Maxillary Sinus Augmentation - Bone Graft Combinations) has designed an elegantly simple experiment. Each patient serves as their own control group - one bone graft mixture goes on the right side of the upper jaw, a different combination goes on the left. Same patient, same healing environment, same immune system, different materials. It's like running an A/B test, except the test subjects are bone cells and the stakes are someone's ability to chew steak again.
After about six months of healing time, researchers won't just eyeball the results and call it a day. They're going full forensic investigation mode - clinical examinations paired with actual tissue biopsies from the grafted sites. They want to know not just whether bone formed, but what quality of bone we're talking about. Because let's be honest, there's bone, and then there's bone.
Why Should Anyone Care About Bone Graft Recipes?
Great question, hypothetical reader I'm pretending asked that. The world of bone grafting materials is surprisingly diverse. You've got autografts (bone harvested from the patient's own body - effective but requires a second surgical site, which is about as fun as it sounds). There are allografts (donated human bone), xenografts (usually bovine or porcine bone - yes, cow and pig bone), and synthetic options made from materials like calcium phosphate ceramics.
Each comes with trade-offs. Autografts are the gold standard because your body recognizes its own tissue, but harvesting it means more surgery, more pain, and more recovery time. Synthetic and animal-derived materials are readily available and don't require additional surgery, but do they perform as well? And what happens when you start mixing and matching?
This is where the research gets genuinely exciting. If we can identify which combinations produce the best quality bone with the fewest complications, we can potentially improve outcomes for the millions of people who need dental implants every year. We're talking about optimizing a recipe that could help grandparents eat corn on the cob again. That's not nothing.
The Bigger Picture: More Than Just Teeth
Dental implants might seem like a purely cosmetic concern - and sure, having a complete smile matters for confidence and self-esteem. But the implications run much deeper (pun absolutely intended).
Missing teeth affect nutrition. People who can't chew properly tend to avoid fruits, vegetables, and proteins in favor of softer, often less nutritious foods. This creates a cascade of health effects that can be especially devastating in older populations already at risk for malnutrition. Restoring the ability to chew isn't vanity - it's healthcare.
The techniques developed for maxillary sinus augmentation also have applications beyond dentistry. Understanding how different graft materials integrate with native bone tissue informs orthopedic surgery, reconstructive procedures after trauma or cancer treatment, and regenerative medicine more broadly. The jaw is basically a very accessible research laboratory for studying bone healing.
What Makes This Study Design Smart
The split-mouth design - where each patient receives both treatments - is a methodological gem. It eliminates so many confounding variables that plague other research. Different patients have different healing capacities, different immune responses, different compliance with post-surgical instructions (we all know someone who would definitely "forget" they weren't supposed to use a straw). By comparing treatments within the same individual, the researchers control for all of that biological variability.
The inclusion of tissue biopsies is equally impressive. Many studies rely solely on imaging - X-rays and CT scans that show bone density but can't tell you much about the actual cellular composition. Are we growing mature, functional bone or just mineralized scaffolding that looks good on a scan? The biopsies will answer that question definitively.
Looking Forward
If this trial demonstrates clear superiority of one bone graft combination over another, it could change clinical protocols worldwide. Dentists and oral surgeons could approach sinus augmentation with greater confidence, knowing they're using the optimal materials. Patients could potentially experience better outcomes and fewer complications.
And honestly? In a world where healthcare often feels like guesswork dressed up in a white coat, studies like this represent the methodical, evidence-based approach we need more of. It's not flashy gene therapy or headline-grabbing AI diagnostics. It's researchers carefully asking, "What if we just... tested which thing works better?" Revolutionary in its simplicity.
So the next time you bite into an apple without a second thought, maybe spare a moment of gratitude for the researchers out there painstakingly comparing bone graft mixtures. They're essentially the general contractors of oral rehabilitation - making sure the foundation is solid before anyone installs the fixtures.
Disclaimer: This blog post is for educational and informational purposes only and does not constitute medical advice. Clinical trials are ongoing research studies, and outcomes are not guaranteed. Always consult with qualified healthcare professionals regarding treatment options. Information about the MSA-BGC Study (NCT07512011) can be found at ClinicalTrials.gov.