
In 5 years, the standard of care for chronic wounds could be a foam bandage that quietly breathes nitric oxide into damaged tissue for over two weeks, no refills needed, no clinic visits required. Here's why.
Right now, roughly 2.5% of the U.S. population lives with a chronic wound. That number jumps dramatically among people with diabetes, peripheral vascular disease, and limited access to regular healthcare. We're talking about wounds that refuse to close for weeks, months, sometimes years - infections that spiral, hospital readmissions that pile up, and medical bills that devastate families who were already stretched thin. If you've ever wondered what a genuine healthcare equity crisis looks like, chronic wound care is a masterclass.
So when a team of researchers publishes a study showing they've engineered a wound dressing that steadily releases a known healing molecule for 17 straight days, my ears perk up. Not because it's a magic bullet (nothing ever is), but because the design philosophy behind it screams "we thought about the people who can't come back to the clinic every 48 hours."
Wait, Nitric Oxide? That Car Exhaust Gas?
I know, I know. Nitric oxide (NO) sounds like something you'd associate with smog reports rather than wound healing. But your body actually produces NO naturally, and it's a workhorse molecule. It fights bacteria. It dilates blood vessels to increase blood flow to injured areas. It signals your immune cells to get to work. It helps new blood vessels form. Basically, NO is the project manager of wound repair, and it's been managing healing long before we figured out what it was doing.
The problem? When you have a chronic wound - especially one complicated by diabetes or poor circulation - your body's natural NO production at the wound site drops off a cliff. The healing project loses its manager, and everything stalls. Researchers have known this for years, but delivering NO in a controlled, sustained way has been the engineering headache that kept everyone up at night. NO is a gas. It's reactive. It doesn't just sit politely in a container waiting to be useful.
Russian Nesting Dolls, But Make It Bioengineering
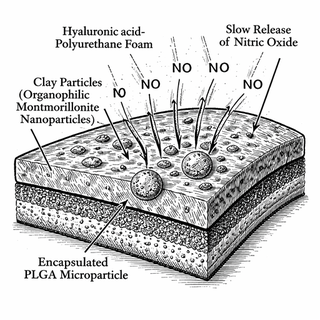
The approach described in this new study is frankly elegant, in that beautifully over-engineered way that makes materials scientists swoon. The team synthesized an NO-donating compound and then tucked it inside organophilic montmorillonite clay nanoparticles - tiny mineral carriers that held onto the NO donor with a loading efficiency of about 79%. Think of it as putting the medicine in a very small, very reliable suitcase.
But they didn't stop there. Those nanoparticles were then encapsulated inside slightly larger PLGA microparticles (about 11 micrometers across, roughly the size of a red blood cell) using a solid-in-oil emulsion technique. So now we've got a suitcase inside a bigger suitcase - a nanocomposite microparticle, if you want the term that'll impress people at dinner parties.
Finally, those microparticles were uniformly dispersed throughout a polyurethane foam matrix infused with hyaluronic acid. The foam is the bandage. The microparticles are the delivery system. And the whole assembly sits on the wound, absorbing exudate like a sponge while steadily releasing NO for up to 17 days.
Seventeen days. From a single dressing application.
Why This Matters for People Who Need It Most
Let's talk about who actually benefits from a wound dressing that works for over two weeks without replacement. It's not the patient with excellent insurance and a wound care clinic ten minutes away. It's the person in a rural community where the nearest specialist is a two-hour drive. It's the elderly patient with limited mobility. It's the uninsured worker who can't afford to take time off for thrice-weekly dressing changes. It's people in low-resource settings globally where wound care infrastructure barely exists.
The beauty of a sustained-release system like this is that it compresses what would normally require multiple clinical visits into a single dressing application. Fewer visits means lower costs, fewer transportation barriers, less time away from work, and - if the results hold up in clinical trials - potentially better outcomes because the wound gets continuous therapeutic support instead of intermittent attention.
The Numbers Under the Hood
The in-vitro results are genuinely encouraging. The foam showed high swelling capacity (meaning it can absorb wound fluid effectively) while maintaining water retention. Mechanical testing confirmed it's tough enough to stay put on a wound without falling apart, and SEM imaging revealed the kind of interconnected porous structure you want for gas exchange and moisture management.
On the biocompatibility front, the foam passed hemocompatibility testing and showed no cytotoxic effects. More interesting still, when human dermal fibroblasts and endothelial cells (the two cell types most responsible for rebuilding tissue and forming new blood vessels) were exposed to the material, they showed enhanced proliferation and migration. In wound healing terms, those cells are the construction crew, and this foam apparently hands them both a blueprint and a strong coffee.
The Honest Caveats
This is an in-vitro study. The foam hasn't been tested on actual wounds in actual humans yet. The leap from "cells in a lab dish migrated faster" to "Mrs. Johnson's diabetic foot ulcer healed three weeks sooner" is enormous. Animal studies will need to come next, followed by clinical trials. The regulatory pathway for a novel NO-releasing wound dressing will be complex, the manufacturing scale-up won't be trivial, and cost-effectiveness analyses will need to demonstrate that the upfront cost of a more sophisticated dressing pays off in reduced overall care burden.
There's also the question of whether 17 days of continuous NO release is the optimal duration and dosing profile for different wound types. A surgical incision, a pressure ulcer, and a diabetic foot wound are very different biological environments with different needs.
But as a proof of concept, this is the kind of work that makes you lean forward in your chair. The engineering is clever, the biological rationale is sound, and the potential implications for health equity are significant. If a single dressing change can do the work of five, we've just removed four barriers to access.
And in chronic wound care, removing barriers might be the most healing thing we can do.
This blog post discusses research findings and should not be taken as medical advice. If you have concerns about wound healing or chronic wounds, please consult a healthcare provider. Research discussed here represents ongoing scientific investigation and clinical validation is still in progress.
All images used in this post are decorative illustrations only and do not represent or reflect the accuracy, reality, or correctness of the referenced research.
Primary Source: A multifunctional hyaluronic acid-polyurethane foam with prolonged nitric oxide release: In-vitro evaluation for wound dressing applications. PubMed: 41941910